Pancreatic Cancer - Pathophysiology, Diagnosis and Staging
*Please note: This slide set represents a visual interpretation and is not intended to provide, nor substitute as, medical and/or clinical advice.
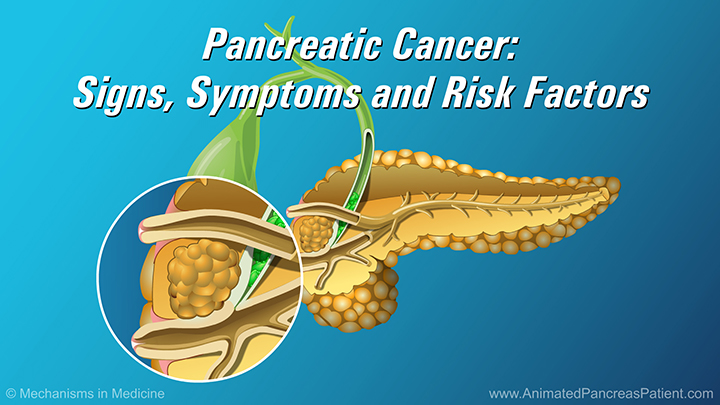
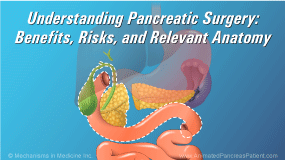
Pancreatic cancer affects the pancreas, a digestive-system organ located in the upper abdomen.
Anatomically the pancreas is divided into three regions: the head, body and the tail.
Cancer is an abnormal growth of cells. Most cancers of the pancreas are adenocarcinomas that arise in the ducts responsible for producing digestive enzymes to break down food. They tend to occur in the head of the pancreas and may grow quickly.
About 10% of pancreatic cancers are endocrine or islet cell cancers. These tend to be more slower-growing tumors located in the body or tail of the pancreas.
Other types of cancers, like lymphomas, sarcomas, acinar cancers and solid and pseudopapillary cancers may also arise in the pancreas.
Pancreatic cancer is diagnosed using imaging and biopsy, following suspicion of the disease based on a set of symptoms.
Initial testing may involve an abdominal ultrasound or a CT scan. Ultrasound uses sound waves to create an image of the structures inside the body, but its information is sometimes limited.
A CT pancreas angiogram scan with IV contrast provides more information. It is more precise and can identify smaller tumors. It can also give an indication of whether the cancer has spread to other organs and what extent of blood vessel involvement is present. An MRI scan may also help clarify the nature of a pancreas mass.
Another increasingly-used imaging technique is endoscopic ultrasound, in which a small probe is inserted into the stomach or small intestine at endoscopy to directly image the tumor.
At the same time, a biopsy, called an FNA (fine needle aspiration) can be performed by inserting a fine needle-like tube into the tumor. The cells removed are then analyzed to see if the tumor is cancerous.
Following imaging, the stage of the cancer is determined. This is based on the size of the tumor and whether the disease has spread to nearby structures (mainly blood vessels) and organs.
Stages I and II refer to localized disease which can only be confirmed by pathologic examination after surgery.
These include small localized tumors in stage I, and in stage II, tumors are seen with (stage IIB) or without (stage IIA) lymph node involvement.
In stage III disease, the tumor is wrapped around or involves important arteries and veins. This means that it can not be removed surgically. This stage is often called locally-advanced.
In stage IV, the cancer has spread to other organs – most commonly the liver or the inner lining of the abdominal cavity, the lungs, lymph nodes or more rarely the bones.
Staging helps doctors determine which treatment approach to take. It also relates to outcomes. Survival rates are higher with stage I and II disease.
This slide show describes pathophysiology, diagnosis and staging of pancreatic cancer.
-
Share with family and friends:
Click here to take our SURVEY
Your feedback is important to us! We will use your feedback to develop future areas of content about pancreatic diseases which will help other patients, caregivers and families.